Herbal Treatment of Major Depression: Scientific Basis and Practical Use
BOOK REVIEW
Herbal Treatment of Major Depression: Scientific Basis and Practical Useby Scott D. Mendelson, MD, PhD; Boca Raton, FL: CRC Press; 2020420 pages • $160.00 (hardcover)
Scott Mendelson, MD, PhD, has written a landmark volume in the Clinical Pharmacognosy series on Botanical Medicines for CRC Press. Why is this a landmark book? It thoughtfully reviews theories of the mechanisms of activity for antidepressants, including ketamine, and lays out the evidence for herbal activity through those mechanisms. Most psychiatrists will be surprised to learn about the anti-inflammatory, antioxidant, anti-diabetic, and neuroplastic effects of these herbs.
Book chapters include relevant in vitro studies of the effects of 66 herbs, providing a foundation for understanding preclinical animal studies and human studies of depression. An additional chapter goes into detail about Chinese Herbal Medicine. Another chapter covers specific plant chemical constituents supported by data on their mechanisms of action. The final chapter discusses how to choose herbs, combine herbs, address comorbidities, and augment conventional synthetic pharmaceuticals.
The evidence base for herbal treatments in depression is now growing rapidly. The availability of quality research should help psychiatrists gain confidence and enthusiasm for prescribing herbs for depression. Those who seek options beyond psychotropic medication will have better choices. Pharmaceutical company researchers wanting to expand their consumer base can develop combination formulas or new herbal products based on data in this volume. Botanical researchers will also find it informative.
Many patients can benefit from herbs with gentler action, fewer adverse effects, and some health benefits beyond their antidepressant effects. Ethnopharmacological differences include heightened sensitivity to adverse medication effects among certain populations. For example, people of Asian ethnicity can be more prone to adverse effects from psychotropics than Caucasians. Consumers who educate themselves about herbal treatments can discuss this knowledge with their healthcare providers.
Another barrier to the use of phytomedicinals is the lack of insurance reimbursement. The out-of-pocket cost must be weighed against the potential therapeutic benefits to the patient, in the context of the patient’s financial situation.
Dr Mendelson succinctly discusses not only familiar herbs for depression, such as St John’s wort and saffron, but also curcumin, lavender, hibiscus, lemon balm, chamomile, and many other lesser known phytomedicinals. He also offers some fascinating clinical pearls, such as the use of milk thistle for obsessive-compulsive disorder (OCD). Data suggesting that St John’s Wort could cause insulin resistance may be news to even experienced herbal prescribers.
When you find that your patient is taking unfamiliar herbs for depression, this is the book to reach for. Here you will find the well-documented, clinically relevant information you will need to evaluate and advise your patient. This will also provide a sound basis for your entry into the realm of herbal prescribing to reduce adverse reactions, minimize the use of synthetic medications, augment other antidepressant treatments, and improve patient compliance and outcomes.
Dr Brown is Associate Professor of Clinical Psychiatry at Columbia University Vagalos College of Medicine, New York.
Experts might read this book straight through, but for those who may not be conversant in biochemistry, the dense structure of the scientific information makes it a heavy read. Most readers will find it an excellent reference book for looking up an herb of interest.
Here and there, editing errors make the text less easy to read. Occasional issues are left out, such as the risk of St John’s Wort causing serious phototoxic rash. For this reason, clinicians should consult more than one source for herbal information, particularly regarding adverse effects.
The clinical utility of the book could have been enhanced by providing some guidance regarding identification of reliable, quality herbal product brands. This is challenging, particularly because companies often change the source or content of their products. This is a difficult and controversial area, but for many herbals, only a few companies manufacture and test their product properly. Furthermore, inferior look-alikes appear to ride on the coattails of high-quality products.
However, these omissions are minor compared to the conceptual and practical steps forward that are represented in this book. Since two thirds of psychiatric patients use alternative approaches, psychiatrists and other health professionals need more information to help patients attain their treatment goals. Phytomedicines can be more helpful than many psychiatrists realize. Overall, they cause fewer adverse effects and are more eco-friendly (causing less pollution than synthetic psychotropics).
I highly recommend this book for psychiatrists and other health professionals treating depression. Furthermore, phytopharmaceutical researchers interested in developing new treatments will find valuable ideas to pursue.
Using Innovation to Reform Medicare Physician Payment
Introduction
Chairman Pitts, Ranking Member Pallone and Members of the Subcommittee – as a practicing physician and Fellow at the Engelberg Center for Health Care Reform at the Brookings Institution, it is a privilege to participate in this hearing today. I commend the Committee for its willingness to confront the difficult issues surrounding Medicare payments to physicians by looking to innovative clinical practices, ideas and solutions.
The current problem of physician payment is not new. Its history can be found in a series of bipartisan legislative efforts aimed at creating a stable system of Medicare physician payment rates and yearly updates to keep health care spending in line with overall economic growth year over year. First, legislation creating the Resource Based Relative Value Scale (RBRVS) was enacted in 1989 and led to the development of relative value units, or RVUs, for each of the physician-related services paid for in the traditional Medicare program. As the number of billable service codes grew over time, an extensive regulatory process was enacted to develop RVU weights and update them year over year. The goal of these updates was to keep the (relative) payments made by Medicare to accurately reflect the value of services.
The problem with this approach is the development of the term “relative.” Over time, the RVU updating system has placed an increasing importance, evidenced by RVU weights, on procedures, scans, and other technical services that fix certain ailments or problems. This has resulted in an emphasis on volume over value and the maintenance of silos in health care, which have eroded the quality of care we deliver to our patients. Non-technical or nonprocedural physician services, including for example “cognitive” services such as spending time with a patient reviewing the risks and benefits of a treatment course or a counseling session to understand health promotion behaviors, have not received significant RVU weight increases over time. Additionally, new services such as email consultations and new approaches to care such as nurse or pharmacist-led care management trams may not be included at all in the list of covered services. These omissions in the RVU system are even more significant as we head into an era of more personalized medicine where the right treatment at the right time for each patient is increasingly individualized-where some patients with heart disease may benefit from a certain imaging procedure but others may not.
The 1997 Balanced Budget Act inadvertently exacerbated the problem with the introduction of the sustainable growth rate or SGR. The SGR was intended to keep the growth in Medicare physician-related spending per beneficiary in line with growth in the nation’s gross domestic product (GDP). In the early years of the SGR, this worked fine, as spending growth was lower than the calculated GDP target and payment rates for physician services increased. But starting with the recession in 2002, spending growth per beneficiary began to exceed GDP growth. In 2002, payment rates were reduced accordingly, by 4.8 percent.
Every year since then, the scheduled SGR payment rate reductions have not taken full effect. Instead, because of concerns about access to care and the sufficiency of payments, Congress has headed off the full payment reductions on a short-term basis. Typically, this has involved offsetting at least some of the budgetary costs with payment reductions affecting other Medicare providers. These short-term patches have not kept up with inflation: between 2000 and 2010, the total cumulative increase in physician payment rates in the Physician Fee Schedule was 8 percent, while the “market basket” for physician services (the Medicare Economic Index) rose 22 percent.[i] As Figure 1 illustrates, actual updates as well as the SGR formula update still grow at rates far below input costs (MEI) and payment rates for other providers, thus exacerbating systemic flaws. The system is broken.
Figure 1: Percent (%) Change of Payment Update Under Multiple Scenarios
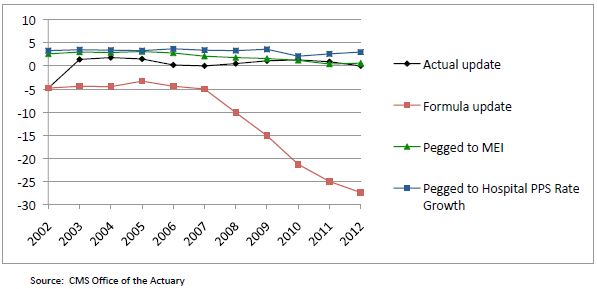
So here we are today, facing yet another possible physician payment cut of 27 percent, and we ask ourselves, “What can be done?” First, we must achieve a long-term vision for payment reform that will help chart a path towards clinician-driven, evidence-based medicine that preserves the autonomy of the physician-patient relationship while moving the profession towards greater accountability. Then, we must look to current innovations, especially those that are clinician-led to help us achieve broader system wide savings.
A Long-Term Vision for Innovation in Physician Payment
The goal of any meaningful Medicare physician payment has to have three essential elements. First, payments must incentivize coordination between providers and across different provider settings. The treatment and management of chronic diseases, acute illness, and prevention and health promotion does not occur within a single physician office or with a single physician or other provider for most individuals. It occurs between specialists in the hospital, in outpatient and rehabilitation facilities, in pharmacies, in community-based organizations, and in the home. The payment system must recognize that incentivizing providers to work together across these divisions is crucial to both the improvement of care for patients and the reduction in unnecessary, redundant, and sometimes harmful or deadly care. Up to $45 billion dollars in health spending each year are attributed to failures in coordination, up to $226 billion in overtreatment and up to $389 billion in administrative complexity.[ii]
Second, payments must inject flexibility into physician practices and clinical processes to remove the sole reliance on the provision of services, tests, and drugs as sources of income. The current fee-for-service model (FFS) incentivizes behaviors that are not in the best interest of patients in many cases and places the emphasis on volume over value and patient-centeredness. In addition, in the era of accountable care—that is, providers being held accountable for the cost and quality of the care that they deliver to patients through financial means—there are numerous elements of care that do not currently fit into the FFS model and are thus uncompensated. Services such as extended office visits, email correspondence, end-of-life counseling, comprehensive treatment plan development and tracking, and critical health IT infrastructure are not part of any fee schedule. Yet these elements of care have been proven to improve the quality of care and lower the overall total cost of care for patients. Any savings from investments made in these areas by providers goes straight to payers.
Third, payments must be tied to appropriate performance and quality measures and embedded into continuous quality improvement programs. This ensures against providers withholding care or providing cheaper care at the expense of patient needs to increase their income. This also reinforces incentives for physicians to adhere to established guidelines, practice evidence-based medicine, and treat patients individually.
With those three elements in mind, it is also important to reinforce that the transition to a new payment system for physician services must occur in stages. A switch to a complete non-FFS system cannot possibly happen in the short term. But it is critical to put into place a process to begin the transition away from a pure volume based, FFS system toward a flexible, blended payment system with payments tied to quality and performance measures, and aligned to coordinated care processes.
At the Engelberg Center for Health Care Reform at Brookings, we have been working with physicians, clinical societies, and other provider groups to start defining the pathway forward, and as a practicing physician, I understand how critical it is to work directly with these groups to make significant progress on this path. We also highlight several key efforts across a variety of specialists with tangible reductions in cost and improvements in quality.
Innovation in the Public Sector
A significant number of important steps to achieve meaningful payment reform have started within the Center for Medicare and Medicaid Innovation (CMMI), including models for bundled payments, coordination among multi-payers in comprehensive primary care and Pioneer Accountable Care Organizations, but I will focus on reinforcing our long-term vision for physician payment by also highlighting where transformation is taking place outside of CMMI. These innovations are noteworthy since in some cases, they have been in place for years with little recognition and acknowledgement by public or private payers. In terms of advancing CMMI’s initiatives, there is broad consensus that the Secretary should advance payment reforms as quickly and responsibly as possible in order to create force multipliers that can achieve the long-term vision outlined above. In particular, I encourage CMMI to identify mechanisms to further their multi-payer efforts such that the important work will transform the delivery system. Finally, the recently announced Challenge Grants offer great insights into clinical innovation. A proposal by Dr. Barbara McAneny of New Mexico Cancer Center (NMCC) was awarded a CMMI grant to expand staff and hours of operation NMCC’s staff and hours of operation to provide an alternative to expensive and inconvenient emergency department services. Under the grant, NMCC will be comparing its quality of care and the cost of care with control-group practices and hospital-based systems. By the end of the third year, Dr. McAneny and her practice colleagues will have a better understanding of all facets of cancer care costs so they can provide a bundled payment mechanism. There is indeed great promise in these examples that should be brought to scale for the nation.
Innovations Informed by Clinical Leadership
Frustrated by the growing cost of care and the scarce time with patients to address important issues, physicians and other clinical leaders are already moving to implement delivery system transformations that are improving care and reducing the total cost of care, many of which are unfunded or uncompensated by payers but still offer the best promise for better care everywhere. Several of my fellow panelists will highlight these efforts.
For example, teams of physicians and health system leaders in Portland, Oregon have implemented an innovative cardiology program led by Drs. Xiaoyan Huang and John Peabody aimed at improving quality, lowering costs and advancing the patient care experience. Known as the Accelerating Clinical Transformation for Cardiovascular Disease (ACT-CVD) Program, the team is redesigning the care of cardiovascular disease by bringing together cardiologists, hospitalists, and primary care providers in a dense urban population in Oregon. Working toward a full-scale system transformation, they have changed care in two general areas: clinical and business. The clinical work has centered on identifying disease specific quality improvements, determining care coordination between specialists and primary care providers, streamlining workflows for high-risk patients, and adoption of appropriate use criteria. The parallel stream of business activities has led to the creation of a large cardiac disease episode of care/bundle to aggregate all cardiovascular costs (approximately $15,000 per patient per year for the high-risk population), the generation of budget expectations for the population, and new physician contract language that incorporates quality and the patient experience. Quality and savings opportunities identified include the following:
The Oregon ACT-CVD program estimates a potential savings of approximately $49.4 million in a target patient population of 77,000 lives connected by hundreds of cardiologists and primary care physicians. But the program still struggles to achieve broad scale largely due to competing incentives in the current reimbursement system—simply put, it is very hard to do this work when the innovations are not recognized by codes, claims, or payers.
Innovation led by physicians is also helping to shape interactions between the multitudes of specialists involved in medical decision-making around cancer care. Dr. John Sprandio, a medical oncologist in Pennsylvania, has changed his practice to promote the concept of a patient-centered medical oncology home (PCMOH). The concept advocates investments in electronic health records, standardization of documentation, physician document review processes, referring/consulting physician access to records, current and longitudinal data reporting, assessment plan development and customization, telephone triage, palliative care programs, and a number of patient tracking processes as the bedrock of their enhanced oncology provider model.[iii] Participation in quality efforts advanced by professional oncology societies gave Dr. Sprandio specialty specific quality metrics to ensure that his care was consistent with the latest guidelines and clinical pathways.
In just five years, Dr. Sprandio’s practice saw significant reductions in both ED visits and hospital admissions leading to significant savings to the system overall, but he faced a dilemma—he was still practicing in a RVU driven, FFS environment that did not necessarily reward any of these innovations, and as a result, there were times when Dr. Sprandio found it challenging to subsidize the coordinated care. Despite this, he persevered. Imagine if payment mechanisms were aligned to incentivize this type of coordination.
Innovation is also occurring in the fields of primary care and other specialties as physicians are consistently voicing concerns that the lack of support for meaningful communication between primary care and specialties results in a breakdown in the management of patients.[iv] A perfect example of an innovative solution to deal with this is in the field of behavioral health care. Patients suffering from depression often fail to seek treatment and primary care physicians often feel overwhelmed with cases that might require more intense monitoring or involvement of an already time constrained and often inaccessible mental health specialist. A multisite effort in the states of Washington , California, Indiana, Texas, and North Carolina (known as the IMPACT Project) aimed to deal with these issues began over a decade ago led by a team of clinicians and quality improvement experts. Primary care practices in eight FFS and capitated settings agreed to engage several depression care managers and a consulting psychiatrist who could electronically review charts and speak with the PCP regarding complex patient treatments. Cost of the care manager and consulting psychiatrist as well as research to study the program’s effects were subsidized by philanthropic foundations and internal resources. The care manager would ensure that close follow-up was scheduled and that care did not “fall through the cracks” as they often do in transitions between primary care and specialties. The consulting psychiatrist worked virtually, covering multiple practices at a time and working over weekends if necessary. Savings of approximately $896 per patient per year were sustained along with demonstrable improvement in mental health outcomes and other indices of chronic disease. Diabetics with depression improved their glucose control. The potential for scale is great, but incentives to change the system are few and far between and all too often, great cost saving opportunities go unrealized.
There are many more examples in additional specialties and primary care—all with the theme that reinforces the need for a payment system that is flexible to innovation but provides a path towards better coordination of care and quality improvement. There will be elements of the FFS system that will need to be retained in this transition and potentially beyond but that should no longer delay progress to achieving better care at a lower cost.
The Importance of Data in Driving Innovation in Medicare Payment
Physicians and other clinicians believe in data informed by evidence and are driven to improve their performance based on high quality data. Perhaps the biggest tool we can give physicians to drive care quality and cost savings is relevant, timely, transparent and actionable data about their patient populations—both clinical and financial. The current state of quality and performance measurement suffers from a few deficiencies. All too often, measures mandated by CMS and other payers are heterogeneous and do not accurately reflect the nature of an individual specialty or population of patients. For example, many of the CMS Physician Quality Reporting System (PQRS) measures are not necessarily broadly applicable to specialties such as oncology or orthopedic surgery, yet these are important specialties which play a significant role in both cost and quality. Expanded efforts to allow registries to qualify for PQRS are a good step, such as those proposed in the recent 2013 Proposed Physician Payment Rule, but must be accelerated to facilitate broader participation and deal with some of the boundaries of claims-based data. The same is true for stage one Meaningful Use Measures—they are essential to usher medicine into the technological age but are largely process measures and not necessarily relevant across health care disciplines. Stage Three Meaningful Use will potentially address outcomes in a more direct manner, but that is yet to be determined. Reporting back to clinicians must also be timely and actionable—this is a promising aspect of the CMMI Pioneer ACO program that is engaged in timely data feeds to clinicians. Receiving patient outcomes data even one to two months much less years later does no good.
An attempt to strengthen significant quality measurement has propelled clinical societies to develop quality improvement programs using unique, clinically vetted, peer-reviewed quality and performance measures. These programs are often completely self-funded, and voluntary from an implementation standpoint, yet have shown incredible promise as vehicles for uniform care improvement and cost reduction. Clinicians developing the measures draw clear lines around conflict of interest and transparency is of the utmost importance. The American Society of Clinical Oncology has developed and refined their Quality Oncology Practice Initiative (QOPI), a clinically approved high-performing set of oncology related practice quality and performance measures. The Society of Thoracic Surgeons (STS) has been a vanguard in developing registry-based quality metrics that have largely moved the profession from great variations in quality and cost to a model for others to follow. Cardiology is doing the same with the National Cardiovascular Data Registry (NCDR), a comprehensive, outcomes-based quality improvement program representing approximately 11 million patient records that can support quality improvement in patients undergoing cardiac catheterization. More examples can be found in other clinical disciplines; a payment system that acknowledges this important work can be paramount in ensuring that a transition from our current payment system to a broader vision can be done with high expectations around quality and measurement reporting.
Supplying Medicare data on these clinician-developed measures and creating a payment system based on performance on these measures over the long term will drive cost reductions and care improvements. Additionally, there are efficiencies of scale to be gained from promoting consistent measures that are developed, collected and reported in a more homogenous manner—practices having to juggle six to eight different quality reporting streams to achieve payment bonuses only exacerbates waste and the silos in health care.
We need to move to a system of quality and performance measurement and reporting that takes advantage of the leadership already shown by many primary care and specialty groups to define unique, clinically approved, appropriate measures; incentivize participation in reporting programs; and, ultimately, move over time to a payment system that rewards high performing providers on these issues and penalizes those who do not.
Moving Forward Now
The path forward is not easy but the opportunity cost of doing nothing is no longer tenable. I hope that I have illustrated that it is feasible to start moving now from payments based on FFS to payments that instead give providers more flexibility to improve the efficiency and quality of their own services, and also to support better coordination, with potential additional support and savings from overall system wide savings. These system wide savings have been well documented and are found in reductions in unnecessary care, administrative simplifications that allow for streamlined quality measurement and transitions in care, timely data reporting, and cost transparencies. It is important to note that while I have focused on examples led by physicians, these are interdisciplinary efforts that reflect the depth and breadth of a great deal of health professions, some of which face significant shortages and supply issues that are significantly affected by disparities in reimbursement.
Thank you again for allowing me to participate in this hearing today and I look forward to further dialogue on this issue.
[i] Centers for Medicare and Medicaid Services Office of the Actuary, accessed July 14, 2012
[ii] Berwick DM, Hackbarth AD. Eliminating Waste in US Health Care. JAMA. 2012;307(14):1513-1516. doi:10.1001/jama.2012.362
[iii] Sprandio J. 2010. Oncology-Patient Centered Medical Home and Accountable Cancer Care. Community Oncology. 7(12):565-572
[iv] Referral and Consultation Communication Between Primary Care and Specialist Physicians: Finding Common Ground. Arch Intern Med. 2011;171(1):56-65.
Research: Paying Attention
By Lisa Fine
May 9, 2001
Julie B. Schweitzer, a psychologist and researcher who studies attention deficit hyperactivity disorder, wants to know how children with ADHD learn differently from those without the disorder.
The answers, she says, are in their brains.
Schweitzer's office at the Maryland Psychiatric Research Center in Baltimore is filled with photographic images from brain scans she has conducted on adults with and without ADHD as they performed mathematical calculations. She says the results, which show that the two groups process information in the brain differently, could help classroom teachers better reach children with the condition.
At a time of unprecedented interest in ADHD, studies of the brain are providing more and more information on how the syndrome works. Schweitzer's work is part of a growing body of scientific research that is helping to identify the biological and genetic underpinnings of ADHD. And such work is being complemented by research using more traditional methodologies, including a major study conducted by the National Institute of Mental Heath on the most effective means of treating it.
Many teachers have come to know the symptoms of ADHD: Students are unable to sit still in their chairs, interrupt class with comments at inappropriate times, or run around the classroom when they are supposed to be sitting at their desks. With about 5 percent of American children diagnosed with ADHD, teachers find themselves on the front lines every day in spotting students who may have the condition and referring them for diagnosis and treatment.
In that role, over the years, educators have been embroiled in controversies over the nature of ADHD, how to treat it, and whether using stimulant medications such as Ritalin is the right course to take. Those debates, which continue to be waged in medical, political, legal, and education policy arenas, have generally been rooted in a lack of consensus on what ADHD really is.
Science Offers Answers
But now, science is beginning to provide some answers. Researchers have already identified which regions of the brain are involved in ADHD, what happens in those regions, how thoughts are processed, and how stimulants affect the brain's functioning. They have also identified genes associated with ADHD and are looking for others in the hope that genetic testing for the disorder won't be far off.
In the past few years, such work has contributed to growing agreement among specialists not only on the biology of ADHD, but also on the best way to treat it.
Findings from that work have the potential to alter debates familiar to educators: whether ADHD exists at all, whether Americans overdiagnose children as having the disorder, and whether such children are overmedicated, to name a few. Those studies and more like them that are in the works could also directly affect how teachers handle students with ADHD in their classrooms.
About 5% of American children are diagnosed with ADHD.
Just three years ago, a panel of medical experts convened by the National Institute of Mental Health to forge a consensus on ADHD called the lack of generally accepted methods of diagnosis, treatment, and follow-up for such children "a major public health problem."
Scientists involved in research aimed at addressing that problem believe that in the next five to 10 years, they will be able to use brain scans and brain imaging to diagnose children with ADHD. Such tests would supplement existing diagnostic methods that rely heavily on reports from parents and educators about children's behavior.
Researchers also say they hope they will be able to determine the exact levels of medication an individual needs, and even develop new medications based on a better understanding of how the brains of people with ADHD work.
'An Ethical Obligation'
Russell A. Barkley, a researcher who has written books on ADHD, says all known causes of the syndrome are biological. He said research has discredited theories that the symptoms associated with the condition are caused by too much sugar, bad parenting, or too much television. Such evidence should reassure school employees who advise parents to pursue a possible diagnosis of ADHD for their children, he adds.
"There is a lot of propaganda out there that might make teachers uncomfortable," says Barkley, the director of psychology and a professor of psychiatry and neurology at the University of Massachusetts Medical Center in Worcester, Mass. "Educators have an ethical obligation, and a duty to play a role in detection and referral of students with ADHD."
ADHD is not necessarily just a disorder of attention, but one also characterized by the inability to control impulsive responses, specialists say. It mars the ability of a person to put off immediate gratification, for instance, in order to experience a greater reward in the long run.
Imaging studies are clarifying which brain regions are involved in the processes that malfunction in people with ADHD. The research suggests two regions strongly involved are the prefrontal cortex, or part of the cerebellum, and at least two of the clusters of nerve cells found deep in the brain, known as the basal ganglia.
Dr. Xavier Castellanos and his fellow researchers at the National Institute of Mental Health found that the right prefrontal cortex and two basal ganglia are significantly smaller in children with ADHD than in those without it. The findings were published in the July 1996 issue of the Archives of General Psychiatry.
The study suggested that the areas of the brain that are reduced in size in children with ADHD are the same regions that regulate attention and impulse control. The right prefrontal cortex is involved in modifying behavior and resisting distractions. The areas of the basal ganglia, called the caudate nucleus and the globus pallidus, inhibit automatic responses and allow more careful deliberation by the cortex, Barkley says.
Thinking Differently
A study of 12 men that Schweitzer conducted from 1997 to 1999 went further to reveal what happens in the brains of subjects with ADHD, compared with those without it, when given a set of mathematical tasks.
She found that the six men with ADHD performed the tasks by visualizing images in their heads rather than hearing the spoken numbers in their minds, the strategy employed by the six subjects without the diagnosis.
In developing her study of adults, which was published in the February 2000 issue of the American Journal of Psychiatry, Schweitzer based her choice of tasks on knowledge that people with ADHD typically have trouble keeping old information in mind while new information is being given to them.
That's why, she says, people with ADHD sometimes blurt out a comment during class, because they fear they might forget it if they wait until someone is finished talking. She says note-taking during lectures presents students with the same difficulty.
So she asked her subjects to listen to a series of numbers. As each number was read, they were supposed to add it to the previous number. For example, if the numbers read aloud were: 1, 2, 3, and 4, the answers would be 3, 5, and 7.
The subjects with ADHD used the occipital regions of their brains, areas associated with visual processing, to perform the task, Schweitzer says. But the subjects without ADHD used the prefrontal cortex, where numbers are remembered, along with the parts of the brain that handle auditory functions.
The men without ADHD performed better on the task, which called for putting aside the total from the previous equation and remembering the previous number in the series before arriving at the next total.
Schweitzer says the subjects with ADHD were more inclined to add the new number spoken to the total of the two previous ones, rather than the previous number in the series. The task was difficult for them because it involved repeatedly "switching gears," she explains. That finding is consistent with the frequently observed difficulty that students with ADHD have in making transitions from one activity to another, she adds.
Another finding was that, over time, the men without ADHD needed less time to come up with the correct answers, and did the equations in a part of their brains that functions more automatically. Because the skill for doing the task was "learned," it no longer required as much effort, and therefore freed their brains up for new tasks.
That didn't happen in the subjects with ADHD, for whom the task did not become automatic.
Classroom Applications Suggested
Schweitzer says she still needs to test more subjects and has a long way to go before drawing specific conclusions on how teachers can better reach students with ADHD.
But one implication of her work, she says, is that "teachers need to remember to use different strategies for different learners. If you give an instruction verbally, maybe you could write it down as well," she suggests.
ADHD is not just a disorder of attention, but also one characterized by the inability to control impulsive responses.
What Schweitzer learned from her study of adult men, which relied on the use of positron emission tomography, often known as PET scans, may hold true for children as well, she says. But because PET scans involve injecting radioactive oxygen into subjects to measure increased blood flows in different parts of their brains while performing a particular task, the test is not used on children.
Schweitzer, an assistant professor at the University of Maryland's Baltimore campus, is about to embark on a study in which she will have children perform the same tasks as the adults in her earlier study. She plans to use a different imaging method more appropriate for younger people with ADHD: functional Magnetic Resonance Imaging, or fMRI, which requires no such injections to measure brain activity.
And she is currently gathering comments from teachers on whether the tasks she is designing will measure a relevant skill that students would use in the classroom.
Examining What Works
Arranging for proper treatment is critical for parents and teachers of children with ADHD, since such youngsters often have a hard time ignoring distractions, sitting still, or thinking before they act, and have trouble completing tasks. If untreated, the disorder can affect a child's ability to make friends or do well in school or in other activities.
Children with ADHD are at risk for depression, lack of self-esteem, and other emotional problems, according to the NIMH.
Last year, the Texas board of education passed a measure recommending that schools consider alternative, nonmedical solutions to behavior problems in the classroom. The Colorado school board took a similar step that year. The Texas measure urged schools to use "proven academic solutions" for dealing with hyperactive students.
But the largest study to date that compared various treatments for the disorder concluded that nonmedical methods were generally not the best course. In 1999, the NIMH's Multimodal Treatment Study of Children with Attention Deficit Hyperactivity Disorder found that medication alone, or medication in combination with intensive behavioral therapy, was significantly superior to other types of treatment.
The study was the first major clinical trial to look at a mental disorder in children, says NIMH spokeswoman Constance Burr. The study involved 18 national ADHD experts who used as subjects nearly 600 elementary school pupils of different socioeconomic backgrounds between the ages of 7 and 9.
Russell A. Barkley,Researcher and professor,University of Massachusetts Medical Center
Researchers randomly assigned the subjects, who participated at six different university medical centers and hospitals in locations including New York, California, Canada, and Pennsylvania, to one of four treatment programs: one that used medication management alone; another that used behavioral treatment alone; a plan that was a combination of both; or routine community care from physicians not involved with the study.
"All children tended to improve over the course of the study, but they differed in the relative amount of improvement," said Dr. Peter S. Jensen, a psychiatrist who was the lead investigator on the study when he was at the NIMH and is now the director of the Center for the Advancement of Children's Mental Health at Columbia University.
"Nonetheless, determining what treatment will be most effective for a particular child is an important question that needs to be answered by each family in consultation with their health-care professional," Jensen said in a statement released with the study in December 1999.
The study concluded that the use of stimulants was more effective than behavioral therapies in controlling the core symptoms of ADHD—inattention, hyperactivity/impulsiveness, and aggression. For anxiety symptoms, academic performance, and social skills, the combination of stimulants and intensive behavioral therapies was consistently more effective.
Still, the researchers involved in the study saw the children for monthly follow-up visits, and gained input from teachers to alter their doses of medicine as needed along the way.
By comparison, the children under the care of community physicians generally saw them face to face only once or twice a year, and for shorter periods of time each visit. The community physicians did not have any interaction with children's teachers, and generally prescribed lower doses of stimulant medication.
NIMH researchers will continue to track the children into adolescence to evaluate the long-term outcomes of those treatments, and will release periodic updates.
Responding to Medication
Methylphenidate, commonly known by the brand name Ritalin, has been used to treat ADHD for 40 years. But only recently has the scientific community begun to understand fully how it works.
In a study published in January of this year, researchers for the first time assessed the effects of therapeutic doses of oral Ritalin on the levels of the neurotransmitter dopamine in the human brain. Dopamine imbalances appear to be closely related to ADHD symptoms.
Although previous research demonstrated that methylphenidate administered intravenously increases dopamine levels in the brain, the new study was the first to assess the effects on dopamine levels when Ritalin is administered orally, the way most patients receive the drug.
No biological test for diagnosing ADHD is currently available.
Using PET scans, a team of investigators from the Brookhaven National Laboratory in Upton, N.Y., and the State University of New York at Stony Brook found that Ritalin increased dopamine levels in the brain.
Researchers at Brookhaven's Center for Imaging and Neurosciences studied dopamine levels in 11 healthy adult males. In two sessions, the volunteers were each given either a placebo or a dose of Ritalin. Based on the men's body weight, the doses were adjusted to correspond to the amounts given to children with ADHD. While their brains were scanned to record dopamine levels, the subjects were asked to rate their feelings of being restless and "high." Meanwhile, physicians monitored each subject's blood pressure and heart rate.
The results confirmed that brain dopamine levels increased significantly about an hour after the subjects swallowed the drug. Those who had taken the placebo showed no such effect. The study also showed that Ritalin works to suppress "background" firing of neurons that are not needed for performing a particular task. That allows the brain to transmit a clearer signal.
Schweitzer also conducted her test on ADHD subjects who were taking Ritalin, which she predicted would make them use the same parts of their brains to perform the tasks in her study as the subjects without ADHD. That did not turn out to be the case, however.
Ritalin did seem to change the way people with ADHD processed information. Specifically, it appeared to increase activity in certain regions of the brain—for example, the hippocampus, which is used in memory—and at the same time reduced involvement of frontal areas of the brain used in effort.
"With medication, the task was made easier for them," Schweitzer explains.
But a surprising finding from the study was what the medication did not do: It failed to activate the anterior singulate, a part of the brain involved in attention that a person uses for engagement and readiness to focus and act, Schweitzer says.
"I saw that medication helps [people with ADHD] find other, novel pathways, not using traditional regions of the other subjects," she says.
Biological Diagnosis on Horizon?
No biological test for diagnosing ADHD is currently available. Yet earlier this year, a company in Boston offered hopes for a long-sought medical test to diagnose the condition. ("Firm Moves Closer to Brain-Imaging Test for ADHD," March 28, 2001.)
Boston Life Sciences Inc. announced in February that the second of three studies of the company's diagnostic agent, dubbed Altropane, had been successful in identifying adults who had been clinically diagnosed with long-standing ADHD by mapping unusually high levels of dopamine in their brains. Three such studies are generally required by the federal Food and Drug Administration before a company can seek approval to market a product.
Russell A. Barkley,Researcher and professor,University of Massachusetts Medical Center
But the test, which involves injecting radioactive substance, cannot be used on children, says Barkley of the University of Massachusetts, who worked on developing the test. A version safe for children will likely follow, he predicts.
Still, Barkley says, even though a laboratory test is not yet available for ADHD, improved understanding of its biological basis should encourage more people to seek treatment.
"The lack of a lab test right now does not invalidate a disorder," Barkley says. "Most mental disorders do not have one. But what is persistent with ADHD is behavior. Teachers have a strong role in distinguishing that behavior from other children's behavior to identify children with ADHD and get them early treatment."
Barkley believes that in the future, brain scans will be used to diagnose not only ADHD, but also subtypes within the disorder.
According to a report in the March 1999 issue of the New England Journal of Medicine, children who could benefit from medical treatment for ADHD are being missed. That is especially true of girls, who are more likely than boys to suffer from the inattentive subtype of ADHD and therefore lack the tell-tale symptoms of hyperactivity, the report said.
At present, the diagnostic manual of the American Psychiatric Association lists three subtypes: primarily inattentive; primarily hyperactive/impulsive; and a combined type with the presence of both those groups of symptoms.
In light of those variations among individuals with attention problems, more research needs to be done to help educators, parents, and health professionals recognize that every student with ADHD is different and should be treated accordingly, says ADHD researcher Raun Melmed, who speaks to schools, school districts, and conferences about the disorder.
"When you hear a child has ADHD, you think you know what to do just by knowing the diagnosis," says Melmed, the director of the Phoenix, Ariz.-based Melmed Center and a co-director of the Southwest Autism Research Center. "The research is helping us to recognize the individual differences within kids with ADHD. The time has come for education to be far more individualized."
Genetic Research Advances
Research shows that ADHD tends to run in families. Further down the road, researchers hope to create a genetic test for the condition.
Children who have ADHD usually have at least one close relative who also has it. And at least a third of all fathers who showed symptoms of ADHD in their youth have children who display similar behavior. Even more suggestive of a genetic component to the disorder is that when one twin of a pair of identical twins has the disorder, the other is likely to have it, too, according to the NIMH.
Studies have suggested that the disorder could be caused by variations in genes that are active in the prefrontal cortex and basal ganglia. Research has shown the affected genes are likely to be the ones that regulate and transport dopamine, one of the chemicals in the brain called neurotransmitters that help deliver messages from one nerve cell to another.
‘With every research stride taken, we move one step closer toward giving our children a better chance for success.’
Peg Nichols,Spokesman,Children and Adults With Attention Deficit/Hyperactivity Disorder
Genetic researcher James Swanson, a psychologist at the University of California, Irvine, says the research on the genetics of ADHD has leapt ahead of that for other psychiatric conditions.
"Nobody's yet identified a clear gene for depression or other disorders," Swanson observes. "The ADHD area has done that for itself. There is this growing body of work that we can build on."
Swanson says research into the specific areas of the brain and specific functions in those areas involved in ADHD have helped identify "candidate genes," or genes likely to be associated with the disorder.
"When you have these kinds of clues, you don't have do laborious work through all genes to find the ones you want," Swanson says. "It's like knowing the location on an interstate freeway system, with mile markers."
Swanson and a team of colleagues used a candidate-gene approach to confirm that ADHD is associated with genes governing cells that both receive and transmit dopamine in the brain. Their work was published in a 1998 issue of the journal Molecular Psychiatry.
Researchers believe that variations in dopamine receptors or transporters, or both, may result in underactivity of brain regions that are involved in attention and behavior, Swanson says.
Researchers have a long way to go, though, in understanding how exactly genes play a role in ADHD. For example, Swanson says, scientists suspect that genes other than those affecting transmission of dopamine are involved.
"This is just the first step," he says. "It will be a long time before genetic research will be of use to educators."
Researchers are eager for what their future work can tell them about ADHD.
Schweitzer says she is hoping further research can help her determine the exact doses of medication needed to treat children, so doctors will no longer have to rely on trial and error until they prescribe the right amount.
Peg Nichols, a spokesman for Children and Adults With Attention Deficit/Hyperactivity Disorder, a national ADHD advocacy group based in Landover, Md., says more should be done to train teachers and teach parents about the information research has yielded about the condition.
"With every research stride taken, we move one step closer toward giving our children a better chance for success," Nichols says. "Yet equally important, we have to find ways to translate the research, bridge the gap between it and real-world practice, and ensure that people who work the front lines—the educators, mental-health professionals, parents, and other caregivers—receive the training, support, and resources they need in order to truly serve the child."
The Research section is underwritten by a grant from the Spencer Foundation
Vol. 20, Issue 34, Pages 26-29
Published in Print: May 9, 2001, as Research: Paying Attention
Please enable JavaScript to view the comments powered by Disqus.
Back to Top 

Comments
Post a Comment